For patients suffering from impotence, Viagra’s family of drugs (so-called phosphodiesterase inhibitors 5) are still a treatment option, if not the only one. Drugs are effective in a high percentage of cases, especially where there is a reduced blood circulation, but require administration whenever you want to have a relationship or in any case continuous; In addition, they may be accompanied by important side effects, have a limited duration of action and tend to last for years to be effective because they do not cure vascular disease at this time but limit blood flow to the penis.
When shockwave therapy can be a Viagra replacement?
Some patients with impotence also cannot use these therapies for other health problems; finally, it is estimated that about 50% of patients statistically tend to abandon therapy within a couple of years without renouncing their quality of sexual life. Modern technology comes in handy with the introduction of shocks that have been used in many medical fields for years, from orthopedics to neuro-muscle neurological diseases, to urinary cramps.
Some scientists have deepened the use of this technology in patients with cardiac infarction, in which they want to stimulate regeneration of vessels and, consequently, of the surrounding tissue heart. Low intensity shock waves are capable of inducing neo-angiogenesis phenomena, i.e. regenerating new tissue vessels in the blood.
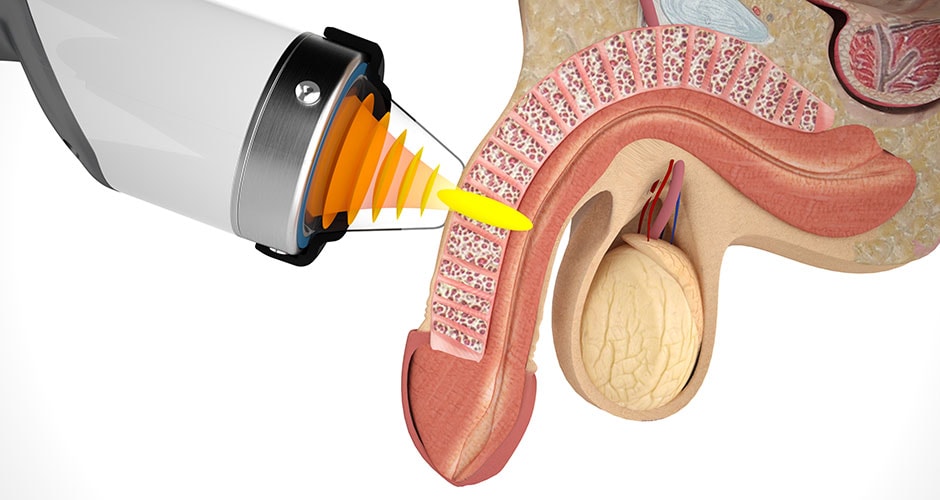
Shock waves in lieu of Viagra
This observation led to the application of the same technology locally at the level of thought in treating erectile dysfunction. Inadequate blood supply to cavernous bodies that produce penile erection is one of the most common causes of erectile dysfunction and increases with age. This technology is simple, painless and leads to lasting success (over two years in 70% of cases) in the treatment of erectile deficit, allowing the patient also not to resort to Viagra family drugs.
It is particularly useful in those cases where pharmacological treatments are discouraged or have proved to be ineffective. Recent scientific evidence suggests that this technology can be successfully used in the treatment of penous plastic injury (Peyronie’s disease) associated with penury incurvation, a disease quite common in the age range of 50 or more years, but often poorly diagnosed and, consequently, , untreated, for the patient’s embarrassment to report the problem to the trusted physician and which, however, can seriously affect the quality of sexual life. The prospect of lasting erection therapy that does not force medication is a major step forward in treating impotence.
Shockwave waves, introduced in medicine at the beginning of the nineties for the treatment of kidney stones (urological lithotripsy), have been used for more than a decade to cure many skeletal musculoskeletal disorders (mainly tendons and bone).
Non-invasive method, shock waves are, in many cases, a valid therapeutic option for the treatment of many diseases, even in acute phase, due to its beneficial anti-inflammatory, anti-ulcer and anti-edema properties (i.e. counteract the ‘swelling’) as well as to stimulate tissue repair. In recent times, they have also proved effective in skin regeneration, accelerating the process of healing wounds, ulcers and ‘hard’ wounds of varying origin, even post-traumatic.
The shock waves are acoustic waves (sound impulses, of a mechanical nature) produced by special generators (lithotrips), and then can propagate into the tissues in a rapid and repeated sequence. They are characterized by a particular waveform (first positive pressure phase, followed by an equally fast, less widespread, negative pressure), which differentiates them from the ultrasound and which, as a whole, is responsible for the positive biological effects applicable in therapeutic fields.
At a microscopic level, pacing with shock waves is comparable to a kind of deep ‘micro-hydromassage’ on tissues and cells that can induce them to react positively with the production of anti-inflammatory substances and factors of growth, which stimulate the regeneration of the tissues themselves, starting from stem cells.
This type of mechanical stimulation can in many cases be successfully applied (in conjunction with other coded therapies) also for the reduction of muscular hypertonia in spasticity of different origin, both lower and upper limbs, partially unknown action. Because of these basic biological effects, the use of shock waves has been widespread for more than a decade, from the urological field to the orthopedic, physiatric and rehabilitative field, but with substantial differences, due to the fact that it acts on living tissues and not on non-vital calcific concretes (such as calculations).
Well-tolerated, non-invasive, repeatable, and clinically effective, the focal waves, in some cases appropriately selected, also prove to be an alternative to surgery, or a post-trauma solution for a trauma or of a surgical procedure itself.
- focal shock waves can act synergistically (i.e., reinforce) with other therapies, or even enhance and accelerate the expected results from surgery;
- the first-rate collision treatment does not preclude the possibility of intervening with other therapeutic solutions (e.g. surgical).
The ways to perform shock-wound therapy are different depending on whether it is bone disorders, tendon and muscular disorders, spasticity, or skin disorders.
The duration of each session may vary from 10 to 15 minutes in the case of soft tissue applications (tendons, muscles and skin), at longer times (up to an hour) for bone treatments.
The patient is usually placed in a supine position on the couch or sitting. Throughout the duration of the therapy, the patient is under constant and direct medical control, so that the level of energy can be adjusted according to the patient’s sensitivity.
Shockwave treatment is a non-invasive, outpatient, safe and proven method. Therapy is virtually free from clinically relevant and well tolerated side effects (if properly performed) as well as repeatable. The benefits that come with it for the patient are now internationally recognized and proven by about 15 years of experience in daily clinical practice.
Last-generation lithotripsy allows to perform all types of treatment currently covered by national guidelines and international:
- lithotripter with electromagnetic generator (suitable for both high-energy and lower-energy treatments on ‘soft tissues’ and especially on tendons)
- lithotripter with ‘defocused’ applicator (indicated for the treatment of tendons, muscles, ulcers, ‘hard wounds’ and painful surgical scars).
Shockwave treatment may, in some cases, have an immediate bleeding effect, but this is not the rule. Generally, the benefits are manifested progressively, with the passing of weeks. In order to properly evaluate the effectiveness of therapy, a follow-up period of about 2-3 months is recommended. During this period will be indicated the abstention from sports activity and rest.
In addition, in the case of treatments for bone consolidation problems (e.g. in pseudoarthrosis), since mechanical stability is essential for healing, an implant dentist or crutches may be prescribed.
Shockwave treatment is effective in treating many bone and soft tissue disorders (tendons, ligaments) due to its beneficial anti-inflammatory, anti-ulcer and anti-edema properties (i.e., to counteract the ‘swelling’) as well as to stimulate tissue repair:
- treatment with shock waves against calcifications
- modulation of shock waves for acute phase inflammatory diseases (i.e., recent onset and already very painful ones)
- treatment of shock waves for the regeneration of tissues (for the treatment of skin ulcers of various origin and related pathologies).
- treatment with shock waves for the treatment of fractures.
Shockwave therapy FAQ
Q: Are shock waves painful or dangerous?
R: No, if performed according to coded therapeutic protocols and with suitable equipment, are generally well tolerated. Especially if it is treatments for ‘soft’ tissue disorders (tendons and ligaments). In some cases, if the patient experiences a slight discomfort, the physician can still measure the energy intensity and the number of blows applied to ensure that the treatment is better tolerated and effective. In addition, some therapeutic protocols provide for a gradual increase in applied energy, enabling the patient to adapt without too much difficulty.
In the case of bone treatments, which apply higher energy and for longer periods of time, pain may be more intense and local anesthesia may be required. Since it is non-invasive, it is safe and almost free of major side effects.
Generally, they can occur after applying high energy:
- small hematomas and superficial and short-lived ecchymosis;
- temporary awakening of painful symptoms. Pain exacerbation after shock waves should not be interpreted as an adverse or negative event, but as a possible positive response to mechanical stimulation of the tissues.
Shockwave treatment is a ‘manu-medical’ therapy, that is, performed by the physician with specific expertise in the subject. Basically, ‘against’ is not the case: like all ‘biological’ treatments that involve tissue response, the result (especially for bone regeneration and, to a lesser extent, cutaneous) is not immediate, but manifests itself over the months following the end of the treatment itself. However, it should be pointed out that shock waves do not replace surgical therapy in all cases.
Q: Does shockwave therapy have contraindications?
R: To date, the following contraindications are recognized, distinct and relative.
They are absolute contraindications:
- the presence of sensitive and sensitive structures, such as an encephalous, spinal cord and gonads in the focal field;
- the presence of tumor and thrombophlebitis pathologies where shock waves should be applied;
These are considered as contraindications:
- the presence of pace maker or electrostimulators of different origin (in particular for patients carrying Pace Maker, one should pay attention to which type of generator to use);
- the proximity of cartilages still under development (in fact this is now considered more a precaution than a true contraindication, as in many experimental studies has been demonstrated the absence of adverse effects)
- blood clotting disorders or changes in blood clotting (coagulopathy with a tendency to bleed): in such cases, the physician will evaluate for each patient whether or not the treatment is appropriate, and possibly the type of instrumentation to be used.
Q: Are the focal waves very painful?
R: No, if performed according to coded therapeutic protocols and with suitable equipment, are generally well tolerated. In some cases, local anesthesia (or sedation only if some types of equipment are used) for bone treatments that require higher energy use may be indicated. The therapeutic procedure with this technology must be performed by a physician with proven experience in this field.
Q: Do the focal waves cause even hematomas?
R: No, if performed correctly and in accordance with the therapeutic protocols indicated for each type of machinery. Any redness and / or skin discoloration are transient phenomena that disappear in 24-48 hours. The appearance of even large hematomas is generally due to improper application of the method, improper use of instrumentation, or severe clotting disorders.
Q: Is the focal wave wavelength repeatable?
A: Yes, some chronic types of pathologies (e.g. plantar fasciitis and rotator cuff pathologies) may require more than one cycle of therapy, especially if the pain persists for some years. In addition, many musculoskeletal disorders, by their very nature, may reoccur over the years, especially in cases where it is not possible to eliminate the cause (e.g. overweight, repetitive efforts, etc.).
Q: Can focal shock waves be applied to acute illnesses?
R: Yes. Early or recently exacerbated acute diseases are generally forms that can potentially benefit from the treatment of focal waves and faster times.
Q: Is the focal waves indicated in all orthopedic pathologies?
R: No, although their field of action has progressively expanded over the years in the musculoskeletal, cure of tendons and bone diseases, such as spasticity, in the area of sores and wounds. Therapeutic indications are generally formulated, not in relation to the anatomical region to be treated, but depending on the origin and nature of the disease. Shockwave cortex waves can in fact be used for ‘healing’ (i.e. healing from inflammation or regenerating tissues), or being used for purely palliative purposes, or in order to obtain, almost exclusively, an anxiolytic effect (painkiller).
Q: Is the focal wave waves ionizing radiation?
R: No, the lithotritor generates shock waves that, as acoustic waves (sound impulses) propagate in an aqueous medium. In addition, there is no additional risk for those who have recently performed radiographic examinations (Rx and TAC) or other instrumental examinations that require the use of ionizing radiation, the same as nuclear magnetic resonance imaging.
Q: Can focal shock waves be applied only in the presence of calcifications?
R: No, the presence of ligamentous or ligated calcifications is not the basic requirement for prescribing collision waves.
Shockwave cortex wounds may, in some cases, at the same time be therapeutic effects, to break down tendon calcifications or near ligaments and joints, by means of a ‘melting’ process (roughly comparable to the action of an anti-lice) of what happens to kidney stones that, with the lithotripter, are crushed.
Q: Is there a risk of injury to bones, tendons, nerves or other anatomical structures?
A: No, proper and competent use of focal waves does not expose to such risks. A precise knowledge of the anatomy of the areas of the body to be treated and an accurate objective examination are required, as well as a specific medical competence in the subject.
Q: Can shock waves also be prescribed for ‘preventive purposes’?
R: No, indication for tendon pathology (so-called ‘soft tissues’) is currently only for symptomatic patients. Bone pathologies may also be indicated to treat asymptomatic patients but with ‘active’ disease, i.e. documentable with instrumental examinations (for example, a slow healing fracture or a bone necrosis).
Q: Do focal waves in some cases be considered the last solution before surgery?
R: Yes. In some tendon pathologies, focal waves may be a viable therapeutic alternative if other treatments have proved ineffective before even offering any surgical intervention.
For some bone diseases, however, as in the case of pseudoarthrosis and necrosis, focal waves are sometimes the first choice treatment.
Q: Is the therapeutic effect of shock waves immediate?
R: No, it is generally necessary to wait a few weeks (even a month or more) before you can properly evaluate the effectiveness of the therapy. It is generally advisable to have a clinical check by the trust specialist 2-3 months after the end of the treatment. It must be borne in mind that, in some cases, an unforeseeable occurrence may occur, in some cases, of an exacerbation of painful symptomatology.
Q: Is it true that focal waves can also be used to regenerate skin tissues?
A: Yes, for some years now, the field of use of this therapy has been extended to the regeneration of ‘skin’, thanks also to technological innovation (tuning of so-called ‘defocused’ shock waves, a variant of the focal shock waves). In all those cases of difficult wound healing, or in the case of wounds and ulcers, the application of defocused shock waves stimulates natural repairing processes, even in the presence of infection. The mechanism of action is related both to the proliferation of new blood vessels and to the stimulation of stem cells.